
We (type 1 diabetics) all have most likely experienced the following at least once during our diabetic career:
ROLLER. COASTER. BLOOD. SUGARS.
Did you know that these rollercoaster blood sugars can speed up how quickly diabetic complications may occur and even death (1)?!
In this post, you’re going to learn:
- Common triggers for rollercoaster blood sugars
- Reasons for their continued presence
- Which is worse: Chronic hyperglycemia or the frequent ups-&-downs of blood glucose levels
Let’s get into it!
What is Glycemic Variability in Type 1 Diabetes?
Glycemic variability is the medical term for the volatile “ride” blood sugars take when they go exceedingly too high or low, then in the opposite direction repetitively.
Gif source: https://tenor.com/b1Kvo.gif
Just like your typical roller coaster!
Glycemic variability has a strong case for speeding up diabetic complications and other illnesses among the general population who have diabetes (2).
The incidence rate for glycemic variability is far greater among type 1 diabetics (42.3%) when compared to type 2 diabetics (26.1%). Rollercoaster blood sugars are also notably the worst among T1D adolescents, as 58% are estimated to experience this (3).
I believe the rate of glycemic variability is much worse among type 1 diabetics, however.
The American Diabetes Association has provided the following A1C goal among most diabetic adults (4):
Less than 7% (154 mg/dL or 8.6 mmol/L)
Meanwhile, here are the estimated rates of how well this goal has been observed (5):
- 17% of diabetic youth have an A1C below 7.5%
- 21% of diabetic adults have an A1C below 7%
- Overall, the average A1C has risen from 7.8% in 2010 – 2012 to 8.4% in 2016-2018
Given that A1Cs are a representation of your average blood sugars for the most recent 2-3 months, these results are either from:
- blood glucose levels that are consistently high
- the average of the blood sugar rollercoaster spikes and drops
- or both
In this post, I’m going to focus mainly on glycemic variability but will later provide medical research to assess which is worse to have.
For those with type 1 diabetes (T1D), glycemic variability can be significant, making management all the more challenging!
How do Rollercoaster Blood Sugars Even Begin?
The first step in glycemic variability is the initial blood sugar spike or drop.
There are multiple ways this can happen.
One of the most common glycemic variability triggers is from either your diet, incorrect insulin dosing, or both after you have a meal:
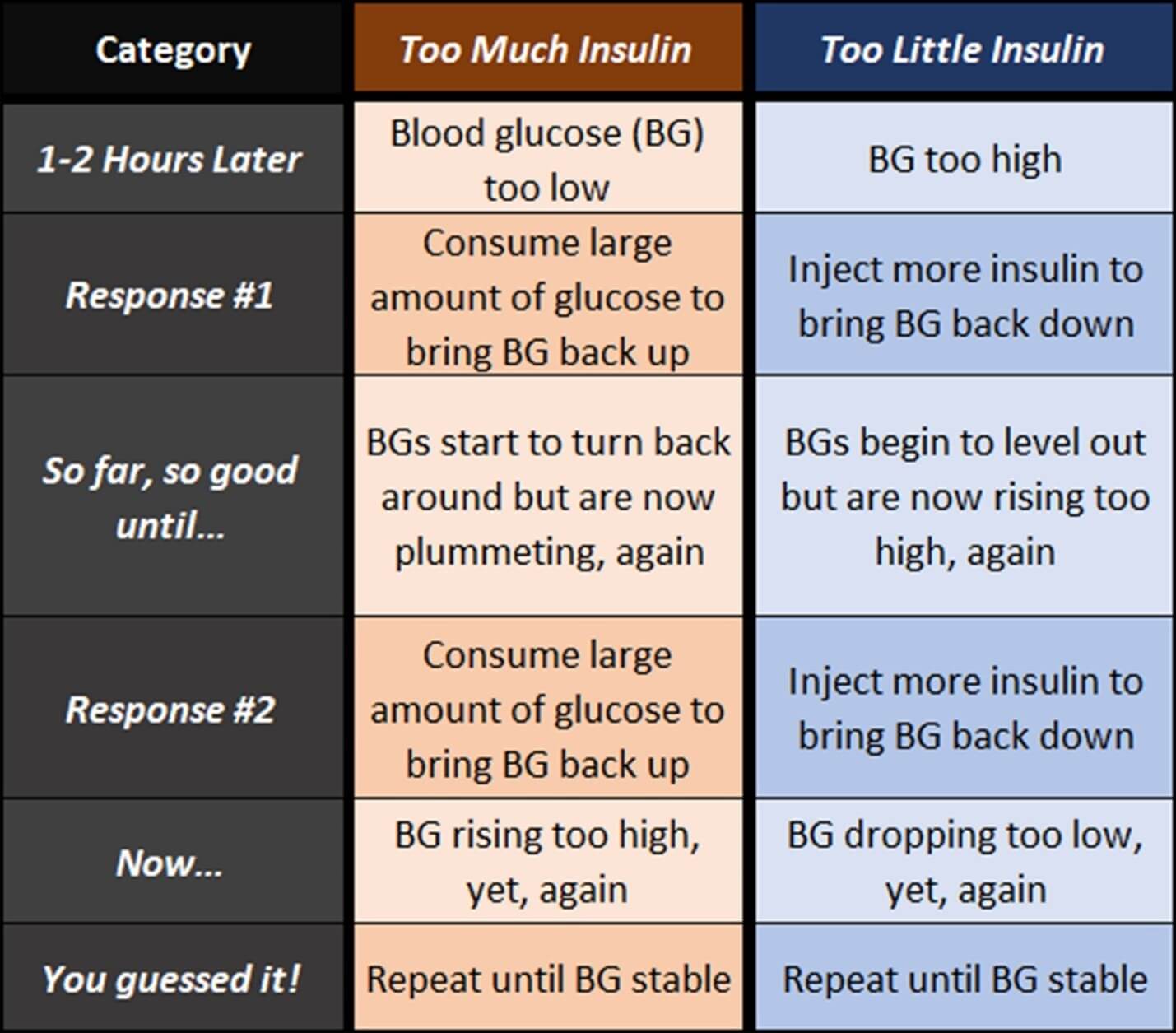 Click image to enlarge
Click image to enlargeI’ve written about particular food choices that commonly set up unreliable calculations for your blood sugar management.
Let’s review other typical causes for rollercoaster blood sugars.
Other Causes for Glycemic Variability in T1D
Remember that glycemic variability begins with a dramatic spike or drop in blood sugar and continues until stable levels are reached.
So, let’s review other common ways sharp BG increases or decreases may occur.
Insulin Absorption Variability
All T1Ds depend on prescribed insulin.
The quicker insulin starts working, the more reliable a type 1 diabetic may be able to predict their blood sugars as needed.
However, should there be a delay in insulin function, this will likely start the first blood sugar spike of glycemic variability.
The absorption rate of injected insulin can vary due to factors like:
- the injection site
- its depth
- blood flow
- if insulin is injected more into fat or muscle
For instance, insulin absorption is usually faster when injected in the abdomen than in your thighs or glutes (6).
Hormonal Fluctuations

I’ve written about the associations between several hormones and glucose dysregulation caused by sleep, physical inactivity, and stress.
Cortisol, adrenaline, glucagon, and growth hormone are just a few that can alter blood glucose levels.
Their secretion patterns, influenced by daily rhythms or stress, can cause an abrupt spike.
A couple of examples include:
- Cortisol is released during a stressful event. As a result, it helps pump glucose into your blood to enable you to fight or flee whatever event is currently present.However, if there is nothing actually to fight or flee from, your blood sugar can spike up.
- Poor sleep can mismatch the timing of melatonin and insulin function, which typically results in higher blood sugars in the morning.
Physical Activity
Exercise increases muscle glucose uptake.
However, its impact on blood glucose is multifaceted.
Moderate activity might lower glucose levels, while intense activity can raise blood sugars or have them plummet!
There’s no 1-size-fits-all regarding a type 1 diabetic’s response to physical activity. However, the more routine it is, the better one is likely able to predict the short- and long-term effects.
There are countless cases when a T1D is exercising or engaging in other physical activity, and their blood sugar either spikes up or down.
Why do blood sugars either go up or down during physical activity?
Assuming BGs have been sustained and stable for at least 2 – 3 hours before exercise and insulin rates are correct:
BG goes up due to cortisol release, triggering glucose to be released into the blood (7).
BG goes down because your muscles take glucose from your blood to replenish energy demands. Incidentally, routine exercise helps increase insulin sensitivity in the musculature among the general population and diabetics (8).
The main activity factors that generally determine these blood glucose results are (9):
- intensity
- time spent performing physical activity
However, remember that many type 1 diabetics will respond differently to the same exercise, intensity, and duration.
Diet
In the chart above, I briefly summarized the effect some meals may have on post-meal blood sugars.
However, the type, quality, amount, and order in which certain macronutrients are consumed combined with other macronutrients may cause different responses.
Another couple of examples include:
- When foods high in fat and carbs are consumed, such as nachos or pizza, the excess of poor fats typically delays carbs from reaching the blood, which can offset insulin rates, leading to unpredictable BG responses (10).This can get even worse by the time carbs reach the blood, as well!
- Consumption of the right kinds of fiber normally lines up along the digestive walls, which are then suggested to help absorb glucose more effectively while limiting the carbs’ effect on your blood sugars (11).This is why eating plenty of protein and fiber before consuming any carbs is recommended, as it’s suggested to lessen insulin demand, glucose spikes, overeating, and weight gain (12).I go over a lot more info on fiber’s importance to a type 1 diabetic here if you wish to check it out.
Illness and Infections
Sickness is commonly paired with hyperglycemia due to the counter-regulatory hormones released during illness (13, 14).
Simply put:
- illness can trigger a stress response, releasing cortisol, which then provokes more glucose in the blood via gluconeogenesis and the liver
- inflammation further impairs blood sugars by releasing cytokines that impair insulin function
- altered eating habits while sick may also contribute to sharp BG changes
Unfortunately, it’s just another vicious circle at work!
Chronic Stress
I’ve written about how chronic stress may directly impair blood glucose stability and indirectly via compromised gut health.
I’ve already summarized cortisol’s involvement.
As a result, these may also be another trigger or a non-helpful addition to influencing rollercoaster blood sugars.
Dawn Phenomenon
Many diabetics experience a surge in blood glucose in the early morning due to the body’s overproduction of glucose sent to the blood.
Over 50% of type 1 diabetics are suspected of being affected by the dawn phenomenon (15).
As a result, this can also trigger glycemic variability episodes if proper diabetic management is inconsistent.
Mechanisms Behind Glycemic Variability
Now that we all know how roller coaster blood sugars commonly begin, let’s get a better idea of what keeps them going while we try to find the balance for our blood glucose levels!
Absence of Normal Insulin Function
Gif source: https://tenor.com/6F7X.gif
In T1D, our pancreas produces far less, if any, insulin due to the autoimmune destruction of our pancreatic β-cells (where insulin is made).
The absence of the body’s natural fine-tuning of glucose levels and reliance on prescription insulin is a primary driver of glycemic variability.
Trust me. I get that it’s not easy thinking like your pancreas:
- 24 hours a day
- 7 days a week, and
- 365 days a year
But these are the cards we’ve been dealt with this disease.
This is why intentional lifestyle behaviors that influence insulin sensitivity typically help to lessen these rollercoaster blood sugars, if not completely.
Real talk:
There’s a saying that I love, and I’ve used this on countless patients to highlight that every choice we make has a consequence and that we all have more power than we genuinely realize in most cases.
In other words, if something is working, then keep up with it. If not? Then, make some new choices!
But everything will stay the same if you do.
And just in case you haven’t heard what many say about insanity:
Gif source: https://tenor.com/bRRdE.gif
Hormonal Counter-Regulatory Responses
In response to low blood sugars (aka hypoglycemia), the body releases glucagon, adrenaline, and cortisol.
These hormones stimulate glucose production, often resulting in a rebound hyperglycemia after a hypoglycemic episode.
At times, this is part of the reason for the dawn phenomenon and why you may wake up in a pool of sweat after realizing hypoglycemia has been going on for longer than it should have been while you were sleeping.
Delayed Gastric Emptying
Up to 58% of type 1 diabetics are estimated to experience gastroparesis, a delay in stomach emptying (16).
This delay is consistent in producing extremely unreliable blood sugar results post-meals.
This is one of the diabetic complications that may arise after the body can no longer handle chronic hyperglycemia.
Also interesting to note is that small intestinal bacterial overgrowth (SIBO) is more commonly seen with gastroparesis (17).
SIBO may very well explain why successfully treating gastroparesis is as complicated as it currently is!
Those of you who have been reading my material for a while shouldn’t be surprised by gut dysfunctions being commonly present among those with autoimmunity and type 1 diabetes (18).
Insulin Resistance
Though more common in Type 2 Diabetes, T1Ds can also develop insulin resistance, requiring more insulin with their blood sugar management.
Research suggests that insulin resistance and glycemic variability are strongly associated with each other (19).
If you’d like more info on insulin resistance and why I believe it’s most likely the reason for holding you and your successful blood sugar management back, check out this series of posts.
Variability in Glucose Uptake
Tissue resistance to insulin can fluctuate due to various factors like a sedentary lifestyle, medications, or even menstrual cycles in women (20).
In the following post, I review the negative effects of sedentary muscle function and its association with troubled blood sugars.
Which is Worse: Rollercoaster or Consistently High Blood Sugars?

Gif source: https://tenor.com/ltUBOyP5gom.gif
Although the average blood glucose level of glycemic variability vs. chronically high blood sugars may not differ, the effects from these average BGs may very well be!
Truthfully, the goal is to avoid both! But when comparing the two, it appears glycemic variability can do much more damage.
Oxidative stress occurs when more free radicals (aka reactive oxygen species or ROS) are present than antioxidants to combat them (21).
This can lead to cellular and tissue damage, contributing to even more insulin resistance and may worsen rollercoaster blood sugars (22)!
Chronically elevated ROS is a popular driver behind diabetic complications, as well (23).
One medical paper suggests that even when average blood glucose levels appear to be controlled, frequent glycemic variability can worsen oxidative stress and increase cardiovascular disease risk compared to chronically high BGs (24).
Another study highlights the following (1, 25):
- given the A1C limitations for health assessment beyond an average BG level for 2 – 3 months, glycemic variability is a more significant and clinically meaningful indicator of diabetic health
- vascular compromise appears to be imminent when rollercoaster blood sugars are routine
- periods of hypoglycemia appear more often with glycemic variability
- those with chronic glycemic variability were found to have a higher death rate than those who did not. This was seen more among hospitalized patients, as well.
Glycemic variability in type 1 diabetes is a multi-faceted challenge resulting from a combination of physiological factors, lifestyle influences, and treatment-related issues.
It’s essential to recognize that while advancements in technology and therapeutics have made it easier to manage T1D, achieving perfect glucose control is still a delicate balancing act.
Each individual’s unique combination of influencing factors makes personalized approaches and continuous education crucial in managing and understanding their own glycemic variability.
What typically further helps is to act on as many factors that influence insulin sensitivity as possible!
Summary
- Glycemic variability is the medical term for the ups-and-downs of blood sugars that commonly occur after meals and inappropriate amounts of insulin bloused
- This occurs in great numbers among type 1 diabetics compared to type 2 diabetics
- Factors that may cause glycemic variability are:
- Insulin absorption dependency
- Hormone imbalances
- Physical activity
- Diet
- Illness and infections
- Chronic stress
- Dawn Phenomenon
- Factors that keep glycemic variability running wild are:
- Absence of normal insulin function
- Hormonal dysfunctions
- Delayed gastric emptying
- Insulin resistance
References
2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10368016/.
3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5846572/
4. https://diabetes.org/about-diabetes/a1c
5. https://www.liebertpub.com/doi/10.1089/dia.2018.0384
6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6079517/
7. https://www.ncbi.nlm.nih.gov/books/NBK538239/
8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3039442/
9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6908414/
10. https://diabetesjournals.org/care/article/36/4/810/37916/Dietary-Fat-Acutely-Increases-Glucose
11. https://diabetesjournals.org/care/article/38/7/e98/30914/Food-Order-Has-a-Significant-Impact-on
12. https://diabetesjournals.org/care/article/41/5/e76/36532/Effect-of-Food-Order-on-Ghrelin-Suppression
13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5716815/.
14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1483173/.
15. https://www.ncbi.nlm.nih.gov/books/NBK430893/
16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2258461/
17. https://pubmed.ncbi.nlm.nih.gov/20085122/
18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6220847/
19. https://pubmed.ncbi.nlm.nih.gov/31707004/
20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8475204/
21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5551541/
22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10253853/
23. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5833737/.
24. https://jamanetwork.com/journals/jama/article-abstract/202670
25. https://diabetesjournals.org/care/article/43/4/821/35722/Respective-Contributions-of-Glycemic-Variability
